Closed Texas Abortion Clinics to Re-Open
By Ellie Politi, 11/9/2014
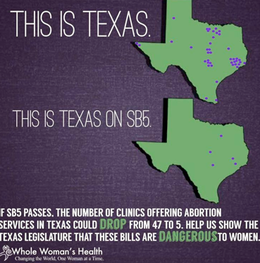
Earlier this month, Texas passed a state law mandating that all abortion clinics meet the same building, equipment, and staffing codes as surgical centers and that all clinic doctors have admitting privileges at a local hospital 30 miles from the clinic. This forced thirteen abortion clinics to shut down over night across the state, leaving only eight open, and questions concerning the constitutionality of the law that affects a population of 5.4 million women able to reproduce have surfaced.
Prior to legislation on October 20, 2014, Democratic state senator of Texas, Wendy Davis, filibustered for eleven hours to prevent the law from being enacted. While the court ultimately passed the law, Davis’ efforts were far from fruitless. Her commitment went viral, and awareness and support were generated across the country.
State proponents of the law have made the claim that this piece of legislation will ensure patient safety and improve quality of care while abortion providers have responded that these new standards are unnecessary and expensive, making it difficult for these clinics to stay open. The New York Times quotes Denise Burke of Americans United for Life, “abortion harms women, and states may regulate in the interest of women’s health.” Abortion providers respond that impeding access to abortion facilities could result in delays in abortion, adversely affecting a woman’s health. In addition, BBC News cites U.S. District Judge Lee Yeakel as having said that these new standards will make an insignificant difference in the already low risk to women.
Also, the inaccessibility of abortion clinics not only poses a physical obstacle to many women but also violates these women’s constitutional rights by doing so. In 1973, the Supreme Court ruled that every woman maintains the right to a pre-viability abortion in the case Roe v. Wade. Judge Yeakel asserts that by obstructing access to abortion clinics, the state is, in effect, denying women their constitutional right.
According to Manny Fernandez of The New York Times, state officials claim that there would not be a significant fraction of women affected if the law were to be enacted; only one out of six women in need of an abortion would live more than 150 miles from the nearest clinic. On the other hand, The New York Times cites Ms. Northup of the Center for Reproductive Rights who states that almost one million women of reproductive age would live more than 150 miles away from the nearest clinic, which in some cases, would make access to these facilities nearly impossible.
The new law also mandates that clinic doctors must have admitting privileges at a local hospital 30 miles from the clinic. State officials claim this to be a necessary precaution for emergency situations while abortion providers see it as an excuse to prevent a clinic from staying open. Since most clinic doctors usually make routine visits to the clinics to perform abortions, they do not often live in the vicinity of the facility. The abortion providers simply see this mandate as an excuse to further discourage the abortion facilities from operating.
The Supreme Court has overruled the law while it is being appealed, so the thirteen clinics have since been reopened, at least temporarily. This law should not be enacted, for there is no medical backing for the implementation. In addition to preventing abortions, this law has other implications. If an abortion clinic cannot afford to operate, its other services, such as cancer screening, HIV screening, counseling, and contraception would no longer be provided. Some of these services provide an imperative resource while others, such as contraception, would just exacerbate the problem of abortion if no longer provided.
Earlier this month, Texas passed a state law mandating that all abortion clinics meet the same building, equipment, and staffing codes as surgical centers and that all clinic doctors have admitting privileges at a local hospital 30 miles from the clinic. This forced thirteen abortion clinics to shut down over night across the state, leaving only eight open, and questions concerning the constitutionality of the law that affects a population of 5.4 million women able to reproduce have surfaced.
Prior to legislation on October 20, 2014, Democratic state senator of Texas, Wendy Davis, filibustered for eleven hours to prevent the law from being enacted. While the court ultimately passed the law, Davis’ efforts were far from fruitless. Her commitment went viral, and awareness and support were generated across the country.
State proponents of the law have made the claim that this piece of legislation will ensure patient safety and improve quality of care while abortion providers have responded that these new standards are unnecessary and expensive, making it difficult for these clinics to stay open. The New York Times quotes Denise Burke of Americans United for Life, “abortion harms women, and states may regulate in the interest of women’s health.” Abortion providers respond that impeding access to abortion facilities could result in delays in abortion, adversely affecting a woman’s health. In addition, BBC News cites U.S. District Judge Lee Yeakel as having said that these new standards will make an insignificant difference in the already low risk to women.
Also, the inaccessibility of abortion clinics not only poses a physical obstacle to many women but also violates these women’s constitutional rights by doing so. In 1973, the Supreme Court ruled that every woman maintains the right to a pre-viability abortion in the case Roe v. Wade. Judge Yeakel asserts that by obstructing access to abortion clinics, the state is, in effect, denying women their constitutional right.
According to Manny Fernandez of The New York Times, state officials claim that there would not be a significant fraction of women affected if the law were to be enacted; only one out of six women in need of an abortion would live more than 150 miles from the nearest clinic. On the other hand, The New York Times cites Ms. Northup of the Center for Reproductive Rights who states that almost one million women of reproductive age would live more than 150 miles away from the nearest clinic, which in some cases, would make access to these facilities nearly impossible.
The new law also mandates that clinic doctors must have admitting privileges at a local hospital 30 miles from the clinic. State officials claim this to be a necessary precaution for emergency situations while abortion providers see it as an excuse to prevent a clinic from staying open. Since most clinic doctors usually make routine visits to the clinics to perform abortions, they do not often live in the vicinity of the facility. The abortion providers simply see this mandate as an excuse to further discourage the abortion facilities from operating.
The Supreme Court has overruled the law while it is being appealed, so the thirteen clinics have since been reopened, at least temporarily. This law should not be enacted, for there is no medical backing for the implementation. In addition to preventing abortions, this law has other implications. If an abortion clinic cannot afford to operate, its other services, such as cancer screening, HIV screening, counseling, and contraception would no longer be provided. Some of these services provide an imperative resource while others, such as contraception, would just exacerbate the problem of abortion if no longer provided.
