How Will the ACA Medicaid Expansion Affect State Budgets?
By Hilary Gelfond
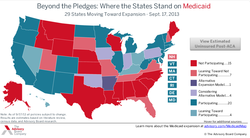
As part of the Affordable Care Act, states are given the opportunity to expand their Medicaid programs to include individuals between 19 and 65 years of age with incomes up to 138% of the federal poverty line (FPL). Despite the opportunity to significantly decrease the proportion of uninsured citizens, 22 states have opted out of receiving virtually “free” money from the federal government. More significantly, the states with the greatest proportion of uninsured poor non-elderly are also the ones who will not expand their Medicaid enrollment. While critics of the program lament that their autonomy in Medicaid decision-making might be breached and that costs will increase, further inspection reveals that there will be little impact from the Medicaid expansion on state budgets.
The federal government will bear 100% of the costs of Medicaid expansion for the first three years. After this, it will bear 90% of total costs. Thus over the first nine years, the federal government will bear a total of 93% of the total cost ($931 billion), while the states collectively will increase spending by $73 billion. Furthermore, the CBO estimates that states will experience a 2.8% increase in Medicaid expenditures above what they would have spent without reform. The Urban institute predicts this figure to be even lower, at 1.4%. However, since the individual mandate will increase the number of Medicaid enrollees regardless of expansion, it is quite possible that the cost of the expansion will be even lower than anticipated.
Under the individual mandate, there is a gap between current Medicaid eligibility and the eligibility for premium and cost-sharing subsidies for private insurance. Thus, people in this gap, a total of 11.5 million people, will remain uninsured. This gap will decrease in states with the expansion, further reducing associated state and local hospital and mental health costs. Furthermore, it is expected that savings will grow over time, as spending on other medical services decreases due to savings from insurance. Other savings will include a $26 to $52 billion decrease in uncompensated care costs and reductions in spending on safety net programs.
Despite the relatively minimal increase in long-term state Medicaid spending demonstrated above, many states overestimate the costs of expansion due to misconceptions about the crowding out of the previously insured, Medicaid participation rates, and costs per new enrollee. In fact, there may be added costs to choosing not to expand Medicaid. Even if states reject expansion, there will still be increased Medicaid participation among individuals who are currently eligible but not yet enrolled. Since these individuals are funded through federal government matching and state inputs, states will incur some costs regardless. Why pay more for the inclusion of these citizens if the government would be willing to pay nearly the full cost through an expansion of Medicaid? Additionally, the Affordable Care Act requires increases in Medicaid payments for certain primary care services through 2014. Many states will continue to offer these same benefit levels after the termination of federal government funding, thus adding to the cost of Medicaid spending. States are exempt from paying this cost if they expand Medicaid services.
Overall, Medicaid expansion will not have any effect on state budgets in the first year of implementation and will only minimally affect budgets thereafter. State concerns about uncontrollable spending under the program are unwarranted, and most likely politically motivated. Upon a pure economic analysis, it is highly beneficial for states to expand Medicaid enrollment under the Affordable Care Act.
Sources:
http://www.cbpp.org/cms/?fa=view&id=3801
http://www.advisory.com/Daily-Briefing/Resources/Primers/MedicaidMap
http://www.nytimes.com/2012/07/15/us/governors-face-hard-choices-over-medicaid-expansion.html?pagewanted=2&_r=0
As part of the Affordable Care Act, states are given the opportunity to expand their Medicaid programs to include individuals between 19 and 65 years of age with incomes up to 138% of the federal poverty line (FPL). Despite the opportunity to significantly decrease the proportion of uninsured citizens, 22 states have opted out of receiving virtually “free” money from the federal government. More significantly, the states with the greatest proportion of uninsured poor non-elderly are also the ones who will not expand their Medicaid enrollment. While critics of the program lament that their autonomy in Medicaid decision-making might be breached and that costs will increase, further inspection reveals that there will be little impact from the Medicaid expansion on state budgets.
The federal government will bear 100% of the costs of Medicaid expansion for the first three years. After this, it will bear 90% of total costs. Thus over the first nine years, the federal government will bear a total of 93% of the total cost ($931 billion), while the states collectively will increase spending by $73 billion. Furthermore, the CBO estimates that states will experience a 2.8% increase in Medicaid expenditures above what they would have spent without reform. The Urban institute predicts this figure to be even lower, at 1.4%. However, since the individual mandate will increase the number of Medicaid enrollees regardless of expansion, it is quite possible that the cost of the expansion will be even lower than anticipated.
Under the individual mandate, there is a gap between current Medicaid eligibility and the eligibility for premium and cost-sharing subsidies for private insurance. Thus, people in this gap, a total of 11.5 million people, will remain uninsured. This gap will decrease in states with the expansion, further reducing associated state and local hospital and mental health costs. Furthermore, it is expected that savings will grow over time, as spending on other medical services decreases due to savings from insurance. Other savings will include a $26 to $52 billion decrease in uncompensated care costs and reductions in spending on safety net programs.
Despite the relatively minimal increase in long-term state Medicaid spending demonstrated above, many states overestimate the costs of expansion due to misconceptions about the crowding out of the previously insured, Medicaid participation rates, and costs per new enrollee. In fact, there may be added costs to choosing not to expand Medicaid. Even if states reject expansion, there will still be increased Medicaid participation among individuals who are currently eligible but not yet enrolled. Since these individuals are funded through federal government matching and state inputs, states will incur some costs regardless. Why pay more for the inclusion of these citizens if the government would be willing to pay nearly the full cost through an expansion of Medicaid? Additionally, the Affordable Care Act requires increases in Medicaid payments for certain primary care services through 2014. Many states will continue to offer these same benefit levels after the termination of federal government funding, thus adding to the cost of Medicaid spending. States are exempt from paying this cost if they expand Medicaid services.
Overall, Medicaid expansion will not have any effect on state budgets in the first year of implementation and will only minimally affect budgets thereafter. State concerns about uncontrollable spending under the program are unwarranted, and most likely politically motivated. Upon a pure economic analysis, it is highly beneficial for states to expand Medicaid enrollment under the Affordable Care Act.
Sources:
http://www.cbpp.org/cms/?fa=view&id=3801
http://www.advisory.com/Daily-Briefing/Resources/Primers/MedicaidMap
http://www.nytimes.com/2012/07/15/us/governors-face-hard-choices-over-medicaid-expansion.html?pagewanted=2&_r=0
