Re-evaluating Schedule I Controlled Substances
In the United States, the Controlled Substance Act gives the Executive branch authority to classify drugs according to their medical uses and the potential for abuse. The Drug Enforcement Administration (DEA) – the federal agency tasked with enforcing controlled substance laws – uses these categorizations, or “schedules” as guidelines for prioritizing enforcement. The Scheduling system is a five-layer hierarchy of risk; Schedule I drugs are defined by their high potential for abuse and lack of accepted medical use while Schedule V drugs are pharmaceutical preparations with limited amounts of controlled substances and the lowest potential for abuse. A prescription can be written for a drug of any schedule other than Schedule I. Despite clearly defined delineations between the schedules, there are glaring inconsistencies.
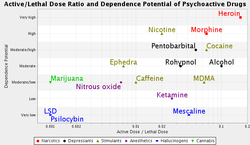
According to the National Institute of Drug Abuse, deaths from pharmaceutical pain medication (individual drugs ranging from schedules II-V) outnumber deaths from all illegal drugs combined. Additionally, the range of relative risk among drugs even within the same schedule is so wide it makes classification seem arbitrary. Heroin and cannabis are both Schedule I even though medical research has shown the former to be physically dangerous, addictive, and a risk factor for HIV and hepatitis while the latter has a range of medical uses with little risk for addiction or negative long-term health effects if used responsibly.
There is a growing movement for legalization of medical cannabis at the state level. Twenty-one states and the District of Columbus have laws allowing and regulating it. This is a good start at highlighting the failures of the current scheduling regime and making policy changes that reduce needless suffering. However, more needs to be done to align drug enforcement with the newest scientific research. Cannabis is not the only Schedule I drug that does not meet its classification criteria. The psychedelic hallucinogens LSD, psilocybin, and mescaline are placed there despite a lack of data indicating risk for abuse. In fact, a recent comprehensive study by Pal-Orjan Johansen of the Norwegian University of Science and Technology found that they are neither addictive nor correlated with mental health problems. In addition to their relative safety as recreational drugs, there is a resurgence of interest in the academic community in their potential for clinical use. There have been studies evaluating LSD as it helps recovering alcoholics stay sober, psilocybin as a tool for aiding with end-of-life anxiety in terminal cancer patients, and MDMA for helping overcome post-traumatic stress disorder.
Drug policy is like any other in that the best policy options stem from informed risk analysis. Unfortunately, the current drug schedules ignore relevant research. It is time to reevaluate drug categorization and enforcement with an emphasis on scientific data and harm reduction rather than an ineffective just-say-no approach.
According to the National Institute of Drug Abuse, deaths from pharmaceutical pain medication (individual drugs ranging from schedules II-V) outnumber deaths from all illegal drugs combined. Additionally, the range of relative risk among drugs even within the same schedule is so wide it makes classification seem arbitrary. Heroin and cannabis are both Schedule I even though medical research has shown the former to be physically dangerous, addictive, and a risk factor for HIV and hepatitis while the latter has a range of medical uses with little risk for addiction or negative long-term health effects if used responsibly.
There is a growing movement for legalization of medical cannabis at the state level. Twenty-one states and the District of Columbus have laws allowing and regulating it. This is a good start at highlighting the failures of the current scheduling regime and making policy changes that reduce needless suffering. However, more needs to be done to align drug enforcement with the newest scientific research. Cannabis is not the only Schedule I drug that does not meet its classification criteria. The psychedelic hallucinogens LSD, psilocybin, and mescaline are placed there despite a lack of data indicating risk for abuse. In fact, a recent comprehensive study by Pal-Orjan Johansen of the Norwegian University of Science and Technology found that they are neither addictive nor correlated with mental health problems. In addition to their relative safety as recreational drugs, there is a resurgence of interest in the academic community in their potential for clinical use. There have been studies evaluating LSD as it helps recovering alcoholics stay sober, psilocybin as a tool for aiding with end-of-life anxiety in terminal cancer patients, and MDMA for helping overcome post-traumatic stress disorder.
Drug policy is like any other in that the best policy options stem from informed risk analysis. Unfortunately, the current drug schedules ignore relevant research. It is time to reevaluate drug categorization and enforcement with an emphasis on scientific data and harm reduction rather than an ineffective just-say-no approach.
